My Cart
You have no items in your shopping cart.


Header Stock photo by © Aldeca Productions | Adobe Stock.
Police as medical first responders, hell yes! Following the tragic 2012 Aurora movie theatre shooting, the Aurora Police Department employed TC3 training (TCC-LEFR) and issued all police officers an IFAK with CAT Tourniquet. The authors here performed a retrospective review of TQ use from 2014 to 2019 in the field.
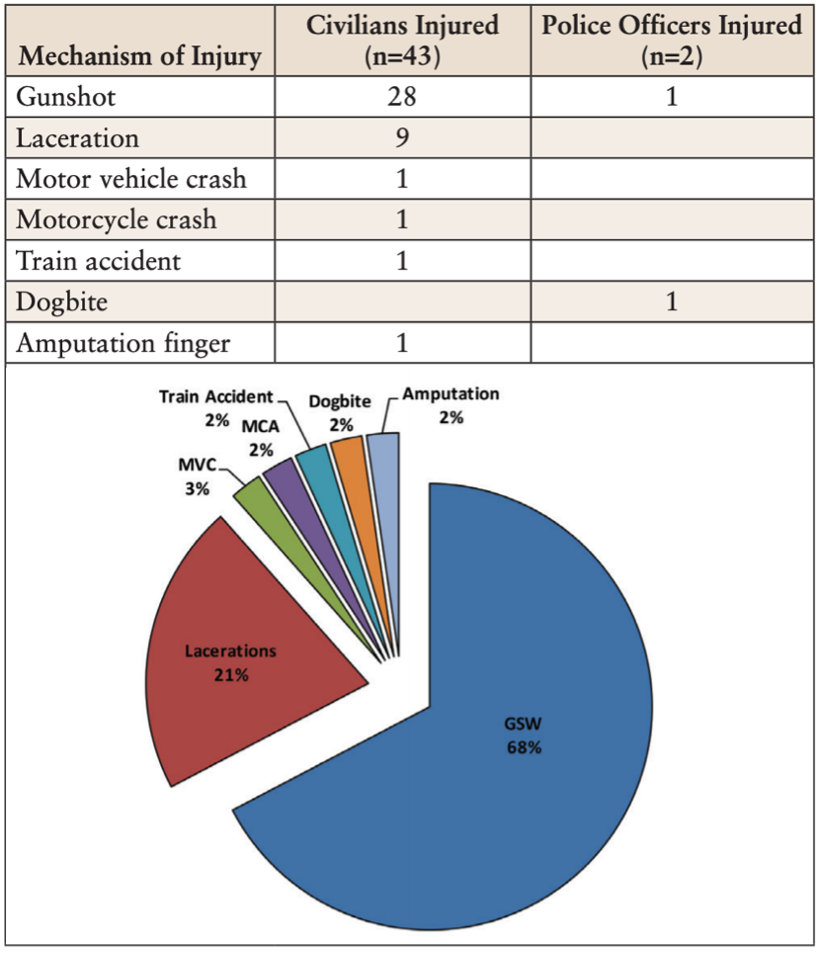
43 incidents where officer recognized an injury with severe blood loss and a TQ was placed. Majority of injuries were gunshot wounds. A few were placed with improper indications (overcalled) which likely had no significant complications given the proximity to Trauma Centers. The authors did not comment/find any missed opportunities(likely due to search criteria). No follow up records were available on the patients. 41/43 were civilian patients while 2 were placed on police officers. Police arrived just over 4 minutes earlier than EMS (ENOUGH TIME TO BLEED OUT). This early hemorrhage control also can occur prior to the patient getting deep into hemorrhagic shock, which reduces mortality from 90% to 10%.
The final consideration was on when to repeat/refresh training. In their observation, officers who were trained up to 6 years prior appeared to continue to retain the skills necessary for proper placement. Given the nature of changing evidence in medicine and TECC guidelines, there likely is a need for refresher training at least every few years.
Other studies have sown somewhat similar results: if you train and equip police properly, they are excellent at early hemorrhage control. They can do this with great accuracy (proper indication) and technique (proper placement).

