
Info from header image by the EMCrit Project, in particular this article talking about how the "Lethal Triad" needs to turn into the "Lethal Diamond."
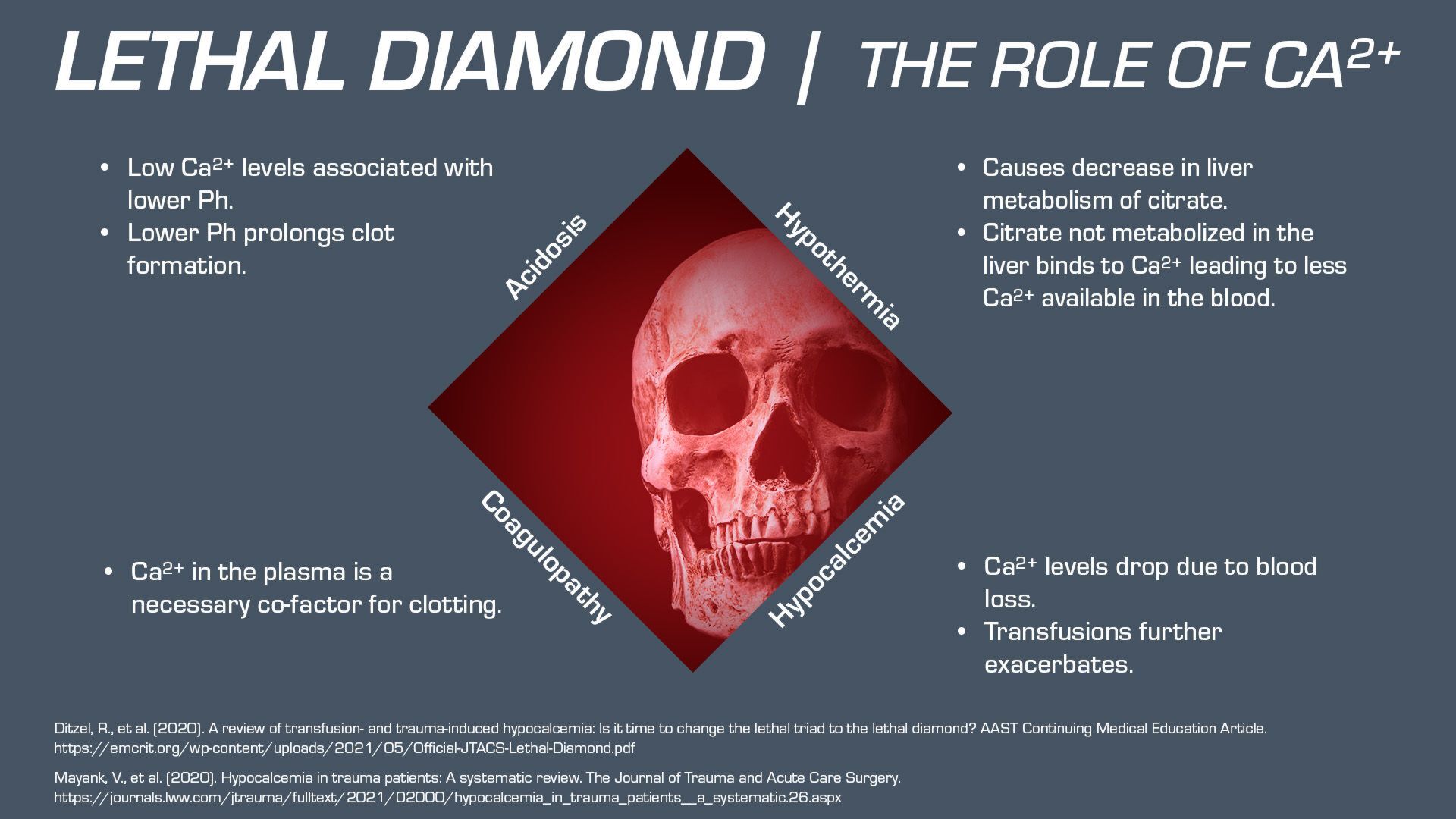
Let’s take a look at an awesome article focused on a hot topic in prehospital trauma. Read the full article at the Journal of Trauma and Acute Care Surgery. For a long time, we have focused on the lethal triad (Hypothermia, Acidosis and Coagulopathy) in trauma patients. Evidence has shown that HYPOCALCEMIA may play a role in mortality of trauma patients. By incorporating HYPOCALCEMIA into the lethal triad, changing it to a diamond, the authors propose that we may affect outcomes by treating HYPOCALCEMIA up front.
| Hypothermia | Acidosis |
|---|---|
| Decreases platelet aggregation, reduces local vasoconstriction, alters enzyme activity in the coagulation cascade, causes leftward shift in oxygen-hemoglobin dissociation curve. | Reduces coagulation factor activity, increases fibrin degradation rate, increases bleeding times. Lower levels of calcium increase acidosis. |
| Coagulopathy | Trauma related Hypocalcemia |
| The failure of blood from the above mechanisms. Extrinsic, Intrinsic clotting pathways rely on calcium so coagulopathy worsens with hypocalcemia. | Decreases cardiac contractility(hypotension). Studies show it occurs in over half of all trauma patients. Hypocalcemia nearly doubles mortality. |
Additionally, Blood Transfusions can worsen hypocalcemia by infusing citrate (calcium binder). 97% of massive transfusion trauma patients become hypocalcemic. Interesting note: packed RBCs contain approximately twice the amount of citrate as Whole Blood.
Treatment: Administering Calcium (10ml Ca Chloride) prehospital can decrease hypocalcemia from 70% to 28%.
JTS Guideline: Administer 1gm Ca up front and then with every 4 units of blood products.
Problem: We don’t know if treating hypocalcemia affects outcome. It makes sense to treat hypocalcemia up front (prehospital) so we should, but we need studies to confirm if it makes a difference.