
How does a Chest Seals Work and Why We Apply Them
Chest seals are designed for a sucking chest wound. What they are is a vented chest seal that allows air to exit from the lungs but prevents air from entering through the lungs. In a casualty with a large open sucking chest wound, air is drawn in through the outside of the lung rather than through the trachea and into the lungs.
As the diaphragm extends down and the ribs expand, air is preferentially pulled into the pleural space from the outside of the chest rather than through the respiratory tract.
So the problem is that air doesn't make it into the alveoli where we have that oxygen exchange.
How to Apply a Vented Chest Seal
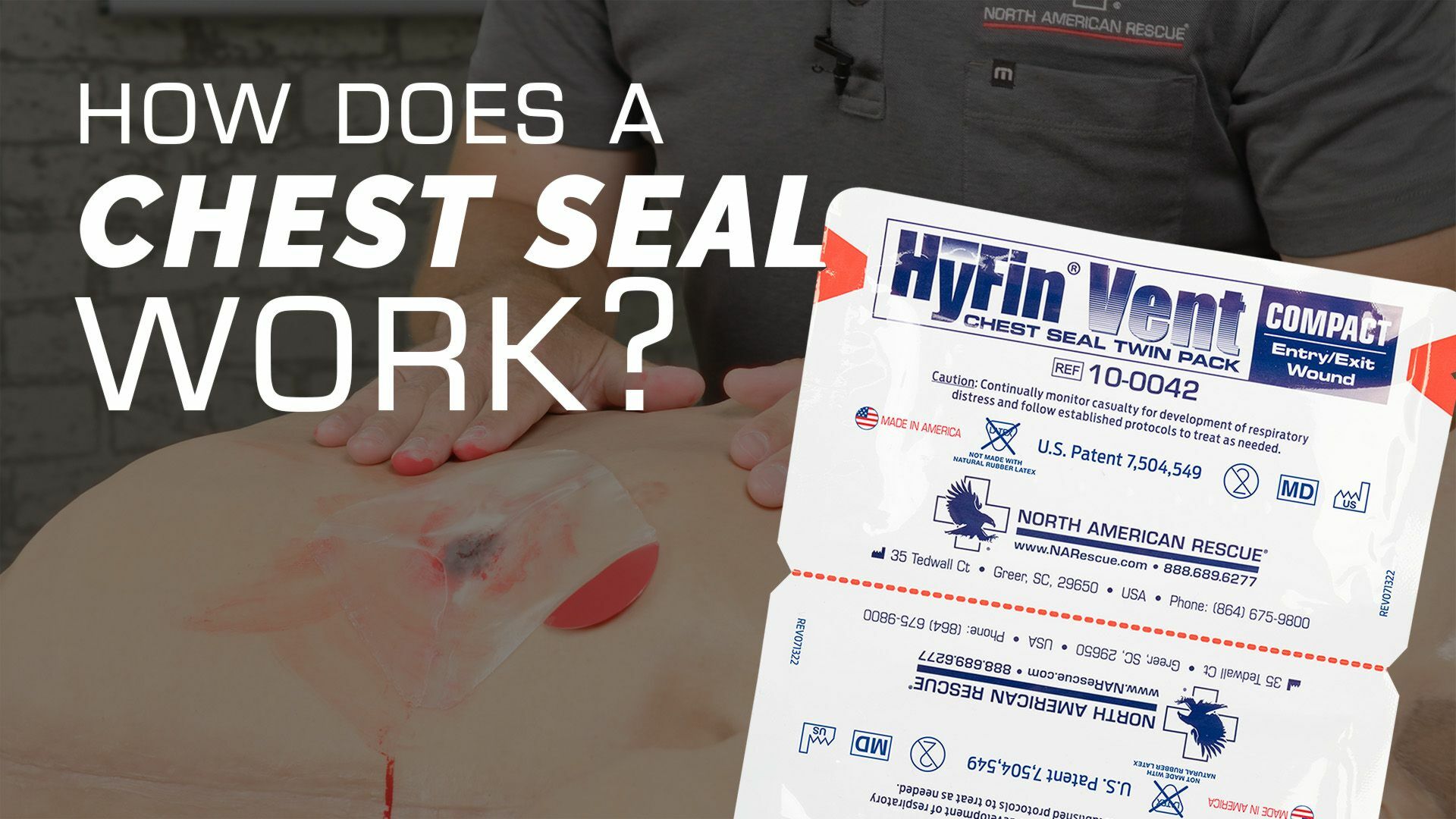
So what I'm going to do is I'm gonna take my chest seal out of here. It's a vented one per the COTCCC recommendations. First thing that I'll do is I'll take this gauze that's included with it.
I'm going to wipe so I get a good seal. I'm going to wipe around it. I'm going to peel off the backing. You need to be careful because this is very sticky. And then you can see here that it's vented and I have these little channels here that'll allow air to escape out so I don't cause a tension pneumothorax.
But when the casualties chest expands, this will flatten out and it'll prevent air from coming in here. Then air goes in the mouth through the trachea, fills up the lungs, and he's able to breathe adequately. So I'm going to place that right over the center. of the wound. Make sure I get a good seal. And now I've got a one way valve here.
So now when the casualty takes a deep breath, diaphragm expands, the ribcage expands out, air can't come in through this way. Instead, it's coming in through his trachea, into his chest, filling up the lungs, and he's able to breathe. Now, always important. We've made an intervention. We've got a significant lung injury.
Monitoring After Chest Seal Application
We want to continue to monitor that casualty, even though it's vented, there's still a potential that they could develop attention pneumothorax. So I'm going to watch that casually. I'm going to monitor him. I'm going to check his vital signs and I'm going to continue to do so. If I believe a tension pneumothorax is starting to develop, that air is expanding outside of the lung in the pleural cavity and collapsing that lung, I can do a couple different things.
And it's going to be based on your medical protocols. The first thing I can do is I can peel this off and I can take a look at that wound. If it's large enough, I might be able to get a fit. finger in there, gloves on, of course, I might be able to get a finger in there and open that up and allow that air to escape.
If that's not working, the next thing I'm going to do is a needle decompression. You can check out some of the other videos on how to do that if your protocols allow you to do that. But that's essentially what burping it is. And then we can go ahead and replace that. And we have our chest seal back on.
So with the vented chest seal in place, now I am preventing air from coming in through the chest every time I casually breathe in, and instead that air is preferentially going in to his mouth, through his trachea. And into the lungs, inflating the lungs. If there's a continued air leak, the vent allows that air to escape in one of three directions.
Reapplying the Chest Seal
Once air is released, I will replace the chest seal to maintain the one-way valve function, ensuring that air is only entering through the trachea, inflating the lungs properly. If air continues to leak, the vented channels in the seal will allow it to escape without causing further complications.
Examining for Additional Wounds
So anytime we have a wound to the chest and we've treated one, we also want to look throughout the rest of the chest up into the armpits or the axilla. I want to roll my casually do it. Good exam along the back and look for any exit wounds or any additional entrance wounds. It doesn't really matter if it's an entry or if it's an exit wound, but I want to identify those and make sure I'm addressing those appropriately.
The Risk of Internal Hemorrhage
The other thing you need to keep in mind is Anytime there's penetrating torso trauma, one of the main problems is going to be internal hemorrhage. You just don't know the path of that projectile took inside the chest. You may be concerned about their respiratory distress, but keep in mind that also might be because they're going into hemorrhagic shock.
Prioritize Evacuation
So anytime we have penetrating torso trauma to the chest or to the abdomen, we need to make sure we prioritize them for evacuation and we want to start treating them for hemorrhagic shock. And that's how and when to apply a vented chest seal for a sucking chest wound.